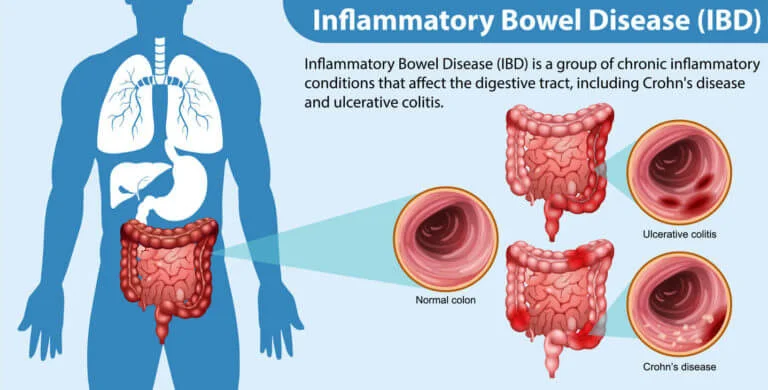
Inflammatory Bowel Disease (IBD) includes two main conditions:
Crohn’s Disease – Affects any part of the digestive tract from mouth to anus.
Ulcerative Colitis – Affects only the colon and rectum.
These are chronic conditions that cause inflammation of the gastrointestinal tract, leading to symptoms like abdominal pain, diarrhea (often with blood), fatigue, and weight loss.
IBD diagnosis requires a combination of tests:
Blood Tests: To check for anemia and inflammation (CRP, ESR).
Stool Tests: To detect infections and inflammation (e.g., fecal calprotectin).
Colonoscopy with Biopsy: Main test to diagnose IBD and distinguish between Crohn’s and UC.
Upper GI Endoscopy: Used if upper tract symptoms are present.
CT/MRI Enterography: For small intestine inflammation in Crohn’s.
Ultrasound: For fast, non-invasive bowel assessment.
Anorectal manometry or defecography (if bowel movement disorders are suspected).
IBD has no complete cure, but modern treatments help control symptoms, reduce flare-ups, and improve quality of life.
5-ASA (Mesalamine) – Mild to moderate ulcerative colitis.
Corticosteroids – Short-term use for flares (Prednisone, Budesonide).
Azathioprine, Methotrexate, 6-MP – Used to maintain remission.
Anti-TNF: Infliximab (Remicade), Adalimumab (Humira)
Anti-integrins: Vedolizumab
IL-inhibitors: Ustekinumab
JAK inhibitors: Tofacitinib (especially in UC)
These target the immune system and are effective in moderate-to-severe IBD.
Antibiotics (for infections or abscesses in Crohn’s)
Iron, calcium, B12, and vitamin D supplements
Anti-diarrheal or anti-spasmodic medications
Diet plays a key role in managing IBD symptoms.
Dietitian-guided meal planning: Low-residue or elemental diets during flares
Nutritional supplements: Protein, vitamins, minerals
TPN (Total Parenteral Nutrition): For severe Crohn’s with malabsorption
Stress management and psychological counseling: Helps reduce flare-ups
Surgery is needed if there is:
Severe bleeding
Strictures (narrowing)
Fistulas or abscesses
Colon cancer risk
Colectomy (removal of colon) – Curative in Ulcerative Colitis
Bowel resection – For damaged areas in Crohn’s
Strictureplasty – Widening narrowed intestines
Ileal pouch-anal anastomosis (J-pouch) – After colectomy in UC
Surgery is not a cure for Crohn’s, but helps manage complications.
Ongoing care is essential due to the chronic nature of IBD:
Regular colonoscopy for cancer screening
Blood and stool tests to monitor inflammation and side effects
Drug level and antibody monitoring (for biologics)
Pregnancy planning and fertility counseling (IBD-specific)
Most IBD treatment centers offer:
24/7 gastroenterologist access during flares
Biologic infusion centers (in-clinic injections/IV biologics)
Emergency care for severe symptoms
IBD clinics with multi-specialty teams (gastroenterologist, surgeon, dietitian, psychologist)
Insurance & cashless claim support
Online consultations and medication reminders
© Copyright 2025 Suraj Hospital All Rights Reserved. Design by Blubuzz Media